Ulcerative colitis (UC) and Crohns disease are grouped under a term called inflammatory bowel disease (IBD). This is characterised by inflammation of the lining of the digestive tract caused by the abnormal immune response of the body
These FAQs aim to answer most asked questions regarding these two diseases and highlight the role of Surgery
Q: What are the similarities and differences between UC and Crohn’s disease?
A: Both UC and Crohns disease are caused by abnormally active immune response of the intestine to the food that we eat. Our digestive tract is a portal of entry of various substances into our body. The lining of the digestive tract has special cells that can activate an ‘immune’ or ‘fighting’ response in reaction to any harmful substances that are ingested. This is a protective function. When this protective action becomes abnormal and the immune response is triggered to even normal food, one gets inflammatory bowel disease.
There are many differences between UC and Crohns. The main difference is that UC can only affect the colon or large intestine, whereas Crohns can affect any part of the digestive system right from the mouth to the rectum/anus.
Q: What are the causes of Inflammatory bowel disease?
A: The exact cause is not known. There is always a combination of various triggering factors –
– Genetic or Hereditary: Having a history of IBD in the family increases risk
– Environmental: Western affluent societies have a higher incidence. However, we are seeing an increasing trend in India, especially with the increasing adoption of Western diet habits
– Diet and lifestyle: Although no specific food has been linked with IBD, eating processed foods and Junk food can increase your risk. Smoking increases the risk of Crohn’s disease.

Q: How do we make a diagnosis?
A: Both UC and Crohns disease need to be diagnosed on biopsy as much as possible. An upper GI endoscopy or colonoscopy can visualise the area of inflamed and abnormal bowel and biopsy can be taken.
Q: Once Diagnosis is made, what is the treatment? Which specialist to consult?
A: The treatment of IBD is planned and implemented by Gastroenterologists. A General physician or GI Surgeon can also initiate the treatment, but a Gastroenterologist needs to be consulted. A variety of treatments are available and new drugs are being researched. Treatment can start with antibiotics, steroids, immune-suppressing drugs, and drugs that modulate the immune response. Injectable medicines and antibodies are used in severe cases.
Q: Do patients with UC or Crohns need to see a surgeon?
A: Yes, around 20-30% of patients with UC and around 80% of patients with Crohns disease will need surgery at some point in their life. A GI/Colorectal Surgeon should be part of the team treating UC and Crohns. A close collaboration between the patient, Gastroenterologist, and Surgeon is essential for best outcomes.
Q: When is Surgery advised for UC or Crohns?
A: Broadly there are these indications
– The disease is severe and cannot be controlled with medicines
– Disease relapse happens very often affecting the quality of life
– Medicines are causing serious side-effects
– There is the development of intestinal cancer, which can happen with long-term IBD
– There is fistula formation from the intestine or the anus
– Emergency situation like intestinal perforation or obstruction.
Q: Can Surgery cure Ulcerative Colitis or Crohns?
A: Surgery can completely cure Ulcerative colitis as this condition affects only the large intestine. Once the entire large intestine is removed, the disease cannot come back.
Surgery cannot cure Crohns disease as it can come back in any part of the intestine, but Surgery can help if a segment of intestine is severely diseased and not responding to treatment. It can reduce reliance on medical treatment.
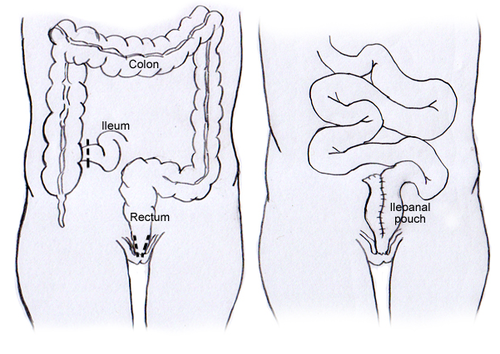
Q: If entire large intestine is removed in UC, how does one pass stools?
A: Once the large intestine is removed, we can create a pouch of the small intestine and join it to the anus. This is called Ileal J pouch surgery. This pouch serves as the reservoir to store stools and adopts to the function of the large intestine over time.
The only other option to pouch surgery is permanent stoma.

Q: Can one lead a normal life after pouch surgery?
A: Yes, there are no major restrictions after pouch surgery. But the frequency of passing stools is higher than normal. Usually, patients with ileal J pouch pass stools 4-6 times in an entire day/night (24 hrs). There are medications which can be used especially while travelling to reduce the frequency.
Q: Can there be complications?
A: Pouch surgery is a highly specialised operation. There are chances of complications such as pouch leak, inflammation etc, these should be discussed with your surgeon before. Pouchitis is a well-known problem which is inflammation of the pouch. It is treatable with medicines.
Q: Does Ulcerative Colitis or Crohns disease increase risk of cancer?
A: Ulcerative Colitis and Crohns disease involving the colon, increases the risk of colon cancer. The risk is usually after 8-10 years following start of the disease, and seen in patients with long-term untreated inflammation of the colon. Therefore, patients with Ulcerative Colitis and Crohns disease need to be on long-term follow-up and have examination at regular interval to detect any cancer or precancerous changes. If diagnosed on time, this cancer is very well treated by Surgery.
Q: What is the aim of treatment?
A: The aim of treatment both in Ulcerative Colitis and Crohns disease is to keep the disease activity at low levels and give the patient a good quality of life. This needs participation of the patient, gastroenterologist, and the GI Surgeon to work as a team to ensure best outcomes. Surgery should not be considered as a failure but an important tool in managing these diseases.